|
|
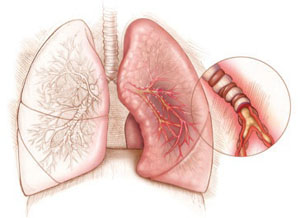
Asthma is a disease of the respiratory system caused by inflammation in the walls of the airways (bronchi), leading to obstruction and their contraction (bronchospasm). This obstruction may be permanent or intermittent, and the symptoms vary from mild, such as fatigue and coughing during laughter or exercise, to more severe, such as persistent cough, difficulty breathing, wheezing, and intense shortness of breath. Diagnosis is usually straightforward and is performed through spirometry. Asthma is a heterogeneous disease, meaning that airway inflammation may be caused by various factors. Therefore, different asthma phenotypes are identified, such as allergic or eosinophilic asthma. When symptoms are suspected, the initial diagnostic evaluation includes spirometry to confirm the disease, followed by assessment of the asthma type, as each type requires a different therapeutic approach. In allergic asthma, it is essential to identify the responsible allergens so that treatment can be appropriately adjusted through avoidance or immunotherapy.
Allergic asthma often coexists with other conditions such as rhinitis, rhinosinusitis, and gastroesophageal reflux disease, with rhinitis being the most common comorbidity. The coexistence of these conditions has led to the concept that the upper and lower respiratory tract form a unified system (“one airway disease”). Studies show that 64% of individuals with asthma also suffer from allergic rhinitis, while 20% of individuals with allergic rhinitis also have asthma. Diagnosis of allergic asthma includes a detailed medical history to evaluate symptoms and potential triggers. Spirometry and, if necessary, assessment of bronchial hyperresponsiveness confirm the diagnosis. If asthma is identified, allergy testing with skin prick tests or measurement of specific IgE in the blood helps identify the responsible allergens. Correlating positive findings with the patient’s symptoms is essential to confirm the allergic origin.
|